Last updated on Jul 20, 2026
Home Health Medical Records Audit Form 2013-2026 free printable template
pdfFiller is not affiliated with any government organization
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
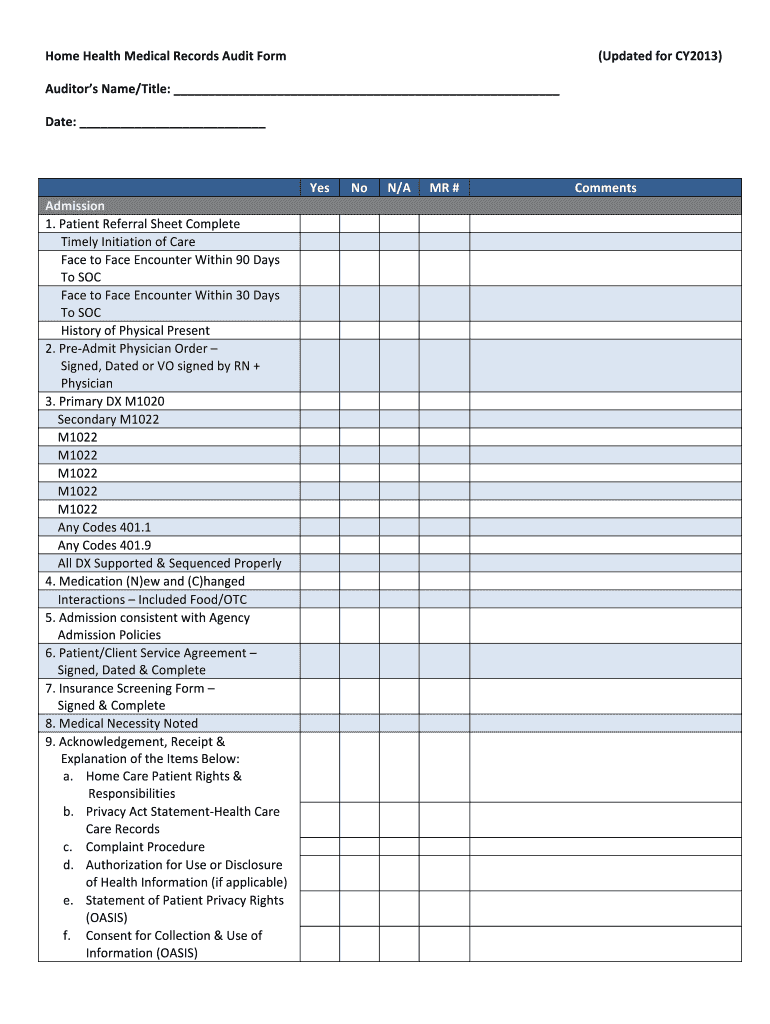
What is Home Health Medical Records Audit Form
The Home Health Medical Records Audit Form is a medical records release document used by auditors to assess patient medical records in home health care settings.
pdfFiller scores top ratings on review platforms
It is the best PDF editor I have come across, great utility and features
It is everything that I needed and more. Thank you
Who needs Home Health Medical Records Audit Form?
Explore how professionals across industries use pdfFiller.

Home Health Medical Records Audit Form is needed by:
-
Home health care auditors
-
Healthcare compliance officers
-
Medical record professionals
-
Healthcare providers conducting audits
-
Patient rights advocates
-
Quality assurance teams
Comprehensive Guide to Home Health Medical Records Audit Form
What is the Home Health Medical Records Audit Form?
The Home Health Medical Records Audit Form serves a critical function in auditing patient medical records within home health care settings. This fillable form provides a systematic approach to ensure compliance and thorough review of medical documentation.
This document is essential for both auditors and healthcare providers, as it enhances the accuracy and reliability of patient records, supporting high standards in care delivery.
Purpose and Benefits of the Home Health Medical Records Audit Form
This form plays a significant role in maintaining healthcare standards through various benefits. It bolsters compliance with home health regulations, ensuring that patient care meets established guidelines.
-
Enhances health care quality through rigorous assessment of patient documentation.
-
Assists in validating medical necessity noted for treatments provided.
-
Supports documentation required for legal, regulatory, and insurance processes.
Key Features of the Home Health Medical Records Audit Form
The Home Health Medical Records Audit Form includes several key features that facilitate effective auditing. These features are designed to streamline the audit process and ensure comprehensive evaluations.
-
Dedicated sections for patient information, diagnoses, and medication records.
-
Utilization of checkboxes, offering options such as yes, no, or N/A for quick responses.
-
Space allocated for auditor comments, capturing specific insights during the audit.
-
Signature and date fields to verify accountability.
Who Needs the Home Health Medical Records Audit Form?
This form is designed for various stakeholders involved in home health care. The primary users include auditors, healthcare providers, and administrators who focus on compliance and quality assurance.
Its importance is particularly evident for those engaged in Medicare and Medicaid compliance, ensuring that home health practices adhere to necessary regulations.
How to Fill Out the Home Health Medical Records Audit Form Online
Filling out the Home Health Medical Records Audit Form digitally can enhance accuracy and efficiency. Here’s a step-by-step guide to assist in the process.
-
Access the form through pdfFiller’s platform.
-
Complete each field meticulously, providing necessary patient information.
-
Use checkboxes for assessments, ensuring you select appropriate options.
-
Add comments where necessary to clarify any observations.
-
Finalize by signing and dating the form before submission.
Review and Validation Checklist for the Home Health Medical Records Audit Form
To ensure the Home Health Medical Records Audit Form is completed correctly, a validation checklist can be invaluable. This checklist aids in verifying the thoroughness and accuracy of all entries.
-
Confirm all mandatory fields are filled out completely.
-
Review for common errors, such as missing signatures or incorrect dates.
-
Conduct a final review to ensure all information is accurate before submission.
Submission Methods and Delivery for the Home Health Medical Records Audit Form
Once completed, there are several methods available for submitting the Home Health Medical Records Audit Form. Each option has its best practices to ensure secure delivery.
-
Submit electronically through a secure online portal.
-
Send a physical copy via registered mail for assurance of delivery.
-
Timing is crucial—ensure that forms are submitted within required deadlines to avoid compliance issues.
Security and Compliance for the Home Health Medical Records Audit Form
Data security and compliance are paramount when managing sensitive healthcare documents. The Home Health Medical Records Audit Form adheres to HIPAA regulations, ensuring patient privacy is respected.
Utilizing tools like pdfFiller enhances document security with features such as encryption, protecting sensitive information throughout the auditing process.
Using pdfFiller for Home Health Medical Records Audit Form
Leveraging pdfFiller for completing the Home Health Medical Records Audit Form can significantly simplify the process. This cloud-based platform offers various capabilities tailored for healthcare professionals.
-
Edit and annotate the form directly within the platform for clarity.
-
eSign documents to ensure timely approvals and streamline workflow.
-
Enjoy the convenience of cloud storage for easy access and sharing while maintaining security.
How to fill out the Home Health Medical Records Audit Form
-
1.To begin, access pdfFiller and search for the Home Health Medical Records Audit Form. Locate it in the template library and open the document.
-
2.Once the form is open, navigate through each section systematically. Use the toolbar to click on checkboxes, where applicable, and type your comments in the designated fields.
-
3.Before filling out the form, gather all necessary information, including patient medical records, admission policies, and assessments. This will ensure accuracy and completeness.
-
4.Carefully review each section of the form, checking off items that are applicable. Ensure that all necessary sections are filled out based on your audit findings.
-
5.Once you have completed all fields, take a moment to review the entire form for any errors or omissions. Make corrections as needed to guarantee that all required information is accurate.
-
6.After finalizing the form, save your progress by selecting the ‘Save’ option which stores your completed document in your pdfFiller account.
-
7.Finally, download a copy of the form to your device or submit it directly through pdfFiller, depending on your organization’s protocol for document submission.
Who is eligible to use the Home Health Medical Records Audit Form?
The Home Health Medical Records Audit Form is designed for auditors and healthcare professionals who conduct audits of patient medical records in home health settings.
What information do I need to complete the form?
Before completing the form, gather essential information about the patient’s medical records, admission policies, diagnoses, and any previous assessments to ensure accurate reporting.
How do I submit the completed audit form?
After completing the Home Health Medical Records Audit Form on pdfFiller, you can submit it either electronically through the platform or print it out for manual submission, based on your organization’s requirements.
What are common mistakes to avoid when filling out the form?
Common mistakes include missing signatures, failing to provide comments for unchecked items, and not reviewing the form for accuracy before submission. Ensure all sections are completed as needed.
Is there a deadline for submitting the audit form?
While there isn't a specific deadline mentioned, it’s important to submit the Home Health Medical Records Audit Form promptly to comply with healthcare regulations and ensure timely audits.
What should I do if I encounter technical issues using pdfFiller?
If you face any technical issues, you can utilize pdfFiller's customer support resources, including tutorials and live help options, to resolve problems swiftly.
What happens after I submit the audit form?
Once submitted, the audit form will undergo a review process by the relevant authorities or management team to ensure compliance and necessary follow-up actions.
Home Health Medical Records Audit Form Form Versions
Related Forms



Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.